

Introduction:
Venous thromboembolism (VTE) is the second most common cause of death in cancer patients next to disease progression. The patients with cancer are not only at increased risk to develop VTE but are also at increased risk of recurrence and bleeding complications from treatment. Hence, anticoagulation is of utmost importance in this population. The International Society of Thrombosis and Hemostasis (ISTH) and American Society of clinical oncology (ASCO) propose guidelines for treatment and prophylaxis of VTE in cancer patients frequently. We aimed to assess the choice and ease among internal medicine residents at different levels of postgraduate training in a teaching community hospital regarding the use of anticoagulation for the prevention and treatment of VTE in medical cancer patients. This study also determines the awareness of the 2019 guidelines of ISTH and ASCO among these residents.
Methods:
A Cross-sectional study including a web-based survey of five clinical scenarios was designed to determine the anticoagulation of choice as per the 2019 ASCO and ISTH guidelines. The scenarios consisted of non-gastrointestinal cancer patients with a diagnosis of VTE with and without normal kidney function, upper gastrointestinal cancer patents with recent VTE, and VTE prophylaxis in hospitalized and ambulatory cancer patients. Also, four questions were included to determine the ease of residents to start anticoagulation in cancer patients and to assess the difference in choices based on their postgraduate year (PGY) level making a total of nine questions.
Results:
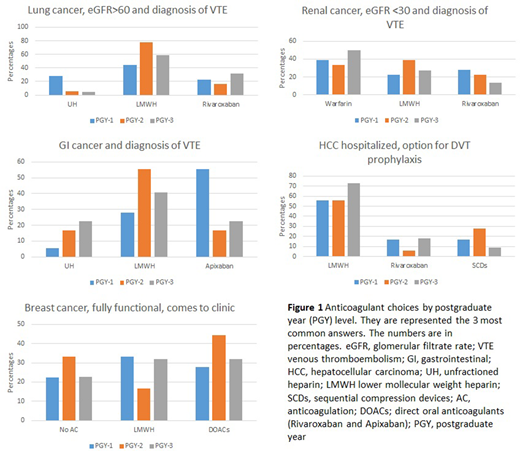
58 (77%) of the total residents (75) responded to the questionnaire who included, 18 PGY-1, 18 PGY-2, and 22 PGY-3. The average correct answers were 1.9 (Mean 39%; SD 21%) out of the five questions that were scored i.e the clinical scenario questions based on guidelines. In the scenario of VTE in non-gastrointestinal cancer, the majority of residents chose Lower Molecular Weight Heparin (LMWH) (60.34%), followed by rivaroxaban (24.14%). For a patient with impaired renal function, although a majority of residents preferred warfarin (41.38%), quite a few picked LMWH (29.31%). For upper gastrointestinal cancer, LMWH was the favored option (41.38%) and apixaban was second (31.03%). For VTE prophylaxis, LMWH had 63.16% of preference vs 35.09% of other options. In an ambulatory, fully functional patient with cancer, only 26% of residents believed anticoagulation is not required. 87.72% of the residents said they were unaware of the current guidelines and a total of 65.38% PGY-3 residents did not feel very comfortable starting anticoagulants on their patients without guidance. For the individual answers based on the PGY level see Figure 1.
Conclusion:
Most of the internal medicine residents preferred LMWH for cancer patients over direct oral anticoagulants. However, they picked the wrong choices in other common scenarios; such as one third preferred to start apixaban in a gastrointestinal cancer patient, or the majority would give prophylactic anticoagulation to ambulatory patients, which is not required per guidelines. These mistakes were supported by the majority of them saying that they were unaware of the treatment recommendations for VTE in cancer patients. Also more than half of the PGY-3 residents are not very comfortable initiating anticoagulants on their own. Based on the above study, we concluded that all residents should be educated on current VTE guidelines on cancer patients, and emphasis should be on including them in the Internal Medicine curriculum. This action will help the residents be more confident and highlight the importance of keeping up with new guidelines.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal